| ..
The
Next Level
Accentuated
Stretch and Flexibility for Classical Dance Development and Martial
Arts (Multi-Sport Olympic Development)
Stephen
M. Apatow, Founder, Director of Research and Development, Sports Medicine & Science
Institute
and International
Dancescience Development Program*
[Vitae][Email]
*
Humanitarian Resource Institute, Humanitarian
University Consortium Graduate
Studies Center for Medicine, Veterinary Medicine and Law.
Introduction
The study guide "Classical Ballet Based Biomechanics:
Orthopedics 101" covers the topic of correct postural
alignment and the mechanical ideal. The general rule is that
any movement pattern outside of correct postural alignment, is stressed
and has the capacity to result in injury. This is a reference
point for postural analysis in dance training and sports specific
development programs. In the context of orthopedic diagnostics,
postural analysis is the key to understanding the mechanism of stress
and substantive course of therapeutic action.
Priority
Focus Areas
Hip Range of Motion: Turnout
Many
dance and sports injuries, related to the demands placed
on the body and requirement for flexibility in concert with poor
warm-up, can produce Achilles, posterior tibial, and patellar
tendinitis. Repeated jolts, with incorrect postural alignment,
contribute to joint complex deformation and the mechanism of injury.
Rule:
Correct alignment = non-stressed, Incorrect alignment = stressed.

|
In the turned out position, the weight should fall from the
body to the thigh and directly through the knee and
ankle. This distribution of weight can be achieved if the
external rotation of the lower extremities occurs at the hip.
As a rule, external rotation of the foot should only occur to (1) the
mechanical ability to track the knee cap over the center line of
the ankle and foot and (2) the center of gravity (vertical axis) 2
inches behind navel, dropping between the heels (1st, 2nd, 4th, 5th).
|
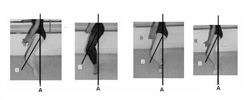
If a child does not maintain correct knee, ankle, foot
alignment, then the bone and articular level will
stabilize into a permanent developmental deformity (knee, ankle, foot
complex).
Understanding
the Mechanism of Injury
To
achieve increased external rotation of the lower extremity, students
may increase their lumbar lordosis or "screw the knee."
Increasing lordosis decreases the tension on the iliofemoral ligament
allowing increased external rotation of the hip. However, it will
put an excess strain on the lumbar spine, as much a the hyperextension
in gymnastics does. "Screwing the knee" is done by assuming a
demiplie (half knee bend) position, allowing the 180 degree positioning
of the feet to be achieved at the floor, then straightening the knees
without moving the feet. This puts
a great deal of torque on the knees and can produce medial knee strain
and patellar subluxation. "Rolling the foot" can produce
posterior tibial tendonitis and bunions.
Knee
Problems
Medial
knee strain is common in student dancers and presents as pain along the
medial side of the knee with no history of specific injury. Pain
is usually worse after class and gradually decreases if there is
a day or two hiatus between ballet classes. There is no history
of swelling or locking. Physical examination often reveals some
tenderness along the medial aspect of the knee but not specifically
over
the joint line or over the medial collateral ligament. No
effusion
is present. Ligamentous laxity, meniscal signs, and patellar
tenderness
are lacking. Radiographs are not usually required in this
situation.
If one finds tenderness specifically along the distal femoral epiphysis
or along the tibial tubercle or patellar tendon, one is dealing with a
different problem. One can confirm the suspicion of medial knee
strain by asking the child to do a plie. An imaginary plumbline
dropped from the knee should land over the second toe. If the
plumbline
falls medial to the foot during plie, then the medial knee structures
are
seeing increased strain and will gradually respond with pain.
Beware
the child who achieves "knees over feet" by assuming a increased
lordotic position.
In
the ballet class, approximately one half to two thirds of class is
spent at barre exercises, most of which include plies in various
positions. In addition, plies are fundamental to initiating jumps
and landing from them. Hence, if one's plie technique is
incorrect, musculoskeletal problems are quite likely. These
problems can be resolved by explaining the proper technique to the
child. The best way for finding a child's proper position using
external rotation of the hip is to have the child stand with his or her
legs straight and feet together. Instruct the child to move his
or her legs from parallel to a position of comfortable external
rotation, keeping the back straight and head up. The "turnout" achieved
will be a function of the child's femoral neck-shaft angle.
Keeping the knees straight will ensure that the rotation will occur at
the hips. Once in this position, the child can be instructed to
keep his or her feet at this angle, but assume the various ballet
positions. While performing plies in these positions, the knees
should fall directly over the feet. Most good ballet instructors
will accept this variation in positioning of their students and realize
that not all students can achieve a 180 degree angle of their
feet. In addition, good instructors will teach the children to
obtain more external rotation using the short external rotators of the
hip rather then cheating with lordosis of the lumbar spine or twisting
the knee.
Patellar
Tendinitis
Patellar
tendonitis, often a part of the presentation of Osgood-Schlatter
disease, is seen in both the young dancer and gymnast. Patellar
tendonitis is also called "jumper's knee" because it is commonly seen
in athletes who jump often. These athletes have pain in the
patellar
tendon unit, either at the distal pole or the patella, along the
patellar
tendon, or on the tibial tubercle.
On
physical examination, one will find very specific point tenderness at
the site of inflammation. Often swelling will be present in the
infrapatellar bursa. The child also may have pain when extending
the leg against resistance. Usually jumping activities are the
cause.
In addition, Micheli (Micheli, L.J., and Rosegrant, S.: Boston
sports medicine: Helping the young athlete. Phys. Sports med.,
9:105-107,
1981) feels that the "overgrowth" syndrome contributes to the
prevalence of Osgood-Schlatter disease in the 11- to 13-year-old age
group. Although children are assumed to be naturally flexible,
poor flexibility and inadequate warm-up were factors in over half the
injuries seen in Micheli's clinic.
The
treatment for patellar tendonitis is rest. The child may do any
activities that do not aggravate the problem. Generally, forceful
kicks, jumps, and plies must be temporarily avoided. Ice massage
over the tendon area will often decrease the pain as well as the
inflammation. In resistant cases, a jumpers knee brace, a knee
sleeve with a pad over the patellar tendon, will decrease the forces
applied to the tendon by the quadriceps muscle and relieve the
pain. Exercising the quadriceps muscle is to be avoided initially
because it will aggravate the problem. However, when the pain has
decreased, one should initiate stretching and strengthening of the
quadriceps. Symptoms generally resolve in
three to four weeks.
Excerpts
from Sports Medicine Concerns in Dance and Gymnastics
Carol
C. Tetz, M.D. Assistant Professor, Orthopedics, University of
Washington, Seattle, Washington
Pediatric
Clinics of North America, Vol. 29, No. 6, December 1982
Clinics
in Sports Medicine, Vol 2, No. 3, November 1983
Part
II: Accentuated Stretch and Flexibility Exercises to Increase Turnout
Most
dancers and athletes don't know that a lack of turnout or hip range of
motion could be caused by soft tissue restrictions, which can be
addressed with an accentuated stretch and flexibility program.
I
personally began dance training in my early 20's, as an athlete training for
international competition in cycling, skiing and rowing. Dance
training was pursued to optimize balance, economy and leverage
mechanics for skating techniques in cross-country skiing. In
conjunction with my sports specific training, my first 3 years
encompassed intensive modern, jazz and ballet (Lee Lund: Jaime Rogers).
In 1987, I progressed to the study of the Soviet System of ballet
training at the Nutmeg Conservatory for the Arts.
My background in studies in sports medicine, exercise physiology and
biomechanics, helped with the analysis of the physical demands of the
dance training, leading to the development of intensive spine and
extremity flexibility programs. In the context of turnout, by the
time I reached Nutmeg Conservatory, I had more turnout that 95 percent
of the students in the development program.
I had a chance to integrate this work with dancers preparing for international ballet competition,
in an experiment that yielded immediate functional improvement of
flexibility (turnout, shoulder complex, spine, extremity) and technical
performance. Shortly thereafter, a general stretch series was
developed for all levels, pre-ballet through upper level.
Hip
Turnout 101
Programs
that do not operate with
students from a one out of a thousand selection process, need to focus
optimization
of the correctable functional limitations. The conventional
approach
is to throw all children into the same training, without regard for
their
lack of prerequisite flexibility, allowing them to advance (in many
cases
deform) to meet the physical demands.
During
international summer programs, upwards of 90 percent of older students
(14-17 years of age) could not parallel plie, with correct alignment of
the kneecap over the centerline of the
ankle and foot. This was due to articular stabilization of the
ankle/knee complex from poor training. The inability to maintain correct
alignment in the parallel, meant that they were not capable of working
in any turned out position without risk of injury. The majority
of these students work with perfect turnout of the feet in the
technique classes, via complete disregard of the alignment problem by
instructors.
Turnout
specific stretch sequences are
classical ballet specific and a fundamental prerequisite for a warmup
progression.
A stretch series that prepares the student for demands of the classical
ballet
training must be completed for a minimum of 30 minutes before every
classical ballet technique class.
Note: Pilates and Yoga do not accomplish the
joint rage of motion needed for the correct execution of classical
ballet
specific training. Stretches must be classical ballet
alignment
specific.
Postural Alignment of the Shoulder Complex and the Mechanism of Joint
Stress and Injury
Postural
alignment of the shoulder complex is one of the most neglected areas,
second to hip turnout, in classical ballet training.
|
Port de bra demonstrating upper
extremity alignment where (1) the shoulder complex is held back and
down, (2)
head of the humorous stabilized as far behind the clavicular head as
possible, (3) major muscle groups include concurrent contracture of the
pectoral and latissimus muscles to stabilize the shoulder complex and
stercliedomastoid muscle for the cervical spine.
The flat back position (non-winged
scapulas), encompasses optimal connection of the arms to the upper
extremity.
|
Shoulder
Stretch
Range
of motion of the shoulder
complex is crucial for correct alignment of the upper extremity.
Holding
a rigid band, rope or pole, position the hands in a position wide
enough (elbows
rotated up in port de bra position),
then progress to a smooth transition overhead. As the range of
motion
opens, bring the hands closer together. Olympic swimmers possess close
to the mechanical ideal, with hands at shoulder width.
Note: The arms must be held straight, with all movements executed below
a threshold of discomfort.
Mechanism of Injury
The
functional arc of elevation of the shoulder is forward with impingement
occurring predominately against the anterior edge of the acromion and
coracoclavicular ligament. 1 As the head of the humorous
bone shifts anterior to the clavicular head, discomfort may be noted
after the exercise and progress to pain during the exercise resulting
in tenderness over the anterior acromion and greater tuberosity.
The dancer or athlete also has a painful or uncomfortable abduction arc
and positive impingement signs. If the bicipital tendon is
involved,
there will be (1) tenderness over the bicipital grove, (2) positive
straight
arm raising, (3) resistive forward flexion at 80 degrees with the elbow
extended, and (4) positive resisted forearm suppuration.
The
differential diagnosis of impingement syndrome includes (1) acute
traumatic bursitis (caused by a direct blow) (2) primary
acromioclavicular pathology (acute tenderness), or a (3) cervical disc
(neck symptoms and nerve involvement beyond the elbow).
The
complaints related to the shoulder complex and bicipital tendon are
generally
responsive to a restriction in activity accompanied by oral
anti-inflammatory
agents.
Ruptures
of the bicipital tendon have been reported in gymnasts, 2
frequently occurring as a degenerative problem or as a consequence
of sudden unexpected stress applied to the contracted biceps.
Symptomatic bursa formation about the scapula raises the traditional
question of
osteochondroma and need for x-ray films to rule out this rare entity. 3
Thoracic
Outlet Conditions
In
thoracic outlet conditions, the neurologic examination is negative and
radiographs normal with the structure involved difficult or impossible
to identify. It is assumed that the ligamentous support structure
or the joints
between the articular processes have been injured and occasionally,
a symptomatic muscle may be indicated.
Treatment
is tailored to the severity of the problem with analgesic,
anti-inflammatory agents, and possibly a soft collar until there is
full, spasm-free
range of motion. In some patients, a specific neck complaint is
accompanied by intermittent numbness, tingling, heaviness, and fatigue
of an upper extremity, which suggests a thoracic outlet syndrome.
The
outlet syndromes are related to lower elements of the brachial plexus
from
C-7 to T-1. X-ray films may reveal a cervical rib with greater
suspicion
attached to the incomplete or short cervical rib due to the congenital
ligamentous bands coupling coupling the cervical rib to the first rib.
Brachial
Plexus Injury
Upper
extremity weakness as a consequence of participation in contact sports
has been associated with injuries to the upper branch of the brachial
plexus as a probable causative neurologic injury. The is
occasioned by downward force upon the shoulder and deviation of the
head and neck backward or toward the opposite shoulder, suggestive of
traction on the brachial plexus. The distribution of nerves from
the upper trunk includes (1) superscapular (supraspinatus and
infraspinatus muscles), (2) upper and lower subscapular (subscapularus
and teres major), musculocutaneous (coracobrachialis and biceps), (4)
axillary (deltoid and teres minor).
Spontaneous
serratus anterior paralysis is a relatively rare condition. A
common cause is backpacking 4 or a brachial neuritis.
The nerve is the most prominent over the second rib and may be injured
by the undersurface of the scapula with forceful pulling of the
arm. It has also been suggested that injury is due to traction
between the point of proximal fixation, the scalenus medius, and its
point of distal fixation, the superior serratus anterior. 5
Neck
Injury
Barre
described a syndrome with symptoms of headache; retro-orbital pain;
vasomotor disturbance of the face ; recurrent disturbances of vision,
swallowing, and pronation due to alterations of the blood flow within
the
vertebral arteries; and associated disturbance of the periarterial
nerve
plexus. The syndrome is one not frequently expressed in
"whiplash" injuries.
Cervical
spondylosis in the middle and distal thirds of the neck is thought to
be the usual provocative cause of irritation of the vertebral arteries.
Limousin has pointed out that in young individuals, congenital
abnormalities of the posterior arch of the atlas, the arcuate foramen,
man produce the symptoms. 6 The possibility can be tested for by
placing the head in a slightly extended position and firmly gripping
the chin. Firm pressure is then exerted between the thumb and
finger, in a gripping action just below and lateral to the occipital
protuberance, at the level of
the lateral masses of the atlas. Pain may be produced by the
pressure accompanied by conjunctival injection and the shedding of
tears. In some cases there will be a feeling of vague faintness.
Since
many of the patients are young anxious and impressionable, assurance
and conservative therapy are generally all that is necessary.
Many of the symptoms are somewhat confusing and suggest a
supratentorial origin, nevertheless, they should be
investigated. Occasionally, more
particularly with additional complaints of dizziness or staggering,
some disturbance in the vestibular aspect may be established by
nystagmography. 7
References
1.
Neer, C.S., and Welch, R.P.: The shoulder in Sports. Orthop. Clin.
North.
Am., 3:583-591, 1977.
2. Del
Pizzo, W., Norwood, L.A., Jobe, F.W., et al.: Rupture of the biceps
tendon in gymnastics. Am. J. Sports Med., 6:283-285, 1978.
3.
McWilliams, C.A.: Subscapular extosis with advetitious
bursa. J.A.M.A., 63: 1473-1474, 1914.
4.
Ilfeld, F.W., and Holder, H.G.: Winged scapula: case occurring in
soldier from knapsack. J.A.M.A.., 120:448-449, 1942.
5.
Gregg, J.R., Labosky, D., harty, M., et al.: Serratus anterior
paralysis in the young athlete. J. Bone Joint Surg., 61A: 825-832, 1979.
6.
Limousin, C.A.: Foramen arculae and syndrome of Barre-Lieou. Int.
Othop., 4:19-23, 1980.
7.
Toglia, J.U., and Ronis, M.L.: Electronytagmograhpy in
clinical and medical legal uses. trans. Pa. Acad. Ophthalmol.
Otolaryngol.,
22-23-27, 1969.
Selected
Bibliography
Agrippina
Vaganova, Basic Principles of Classical Ballet, Dover, 1969
Alfred
A Knopf, The Classic Ballet, New York, 1984
Clinics
In Sports Medicine, Injuries to Dancers ,Saunders
1983
White-Panjabi,
Clinical Biomechanics of the Spine, J.B. Lippincott, 1978
Rosse-Clawson,
The Musculo-Skeletal System in Health and Disease, Harper & Row,
1970
Stanley
Hoppenfeld, Physical Examination of the Spine and
Extremities, Appleton, 1976
Martial
Arts Specific
JudoSport International
"Kokoro"
is a martial arts training system, developed by Stephen M. Apatow, that
integrate classical
biomechanics into judo, ju_jitsu and mixed martial arts disciplines.
Classical
choreographic training used for Olympic development programs in skating
and gymnastics, provides the foundation for skill development. Martial arts provides a
pathway for teaching classical alignment training for sports and
Olympic development programs.
 |
Aspirations
to achieve top level performance requires detailed attention given to
each aspect of the training program. Every day, our diet,
strength, speed, flexibility, postural alignment, mental preparation
and technical training all relate to the factors upon which our bodies
will adapt, to yield our potential performance. -- Stephen M. Apatow
|
|
